Liver Condition Guide
Cirrhosis
Advanced liver scarring requires close monitoring — LiverTracker makes it easier to stay on top of your numbers.
Cirrhosis is the late stage of liver fibrosis where scar tissue replaces healthy liver tissue. While the scarring itself is usually irreversible, early detection of complications and careful monitoring can significantly improve outcomes and quality of life.

Understanding Cirrhosis
Cirrhosis develops when chronic liver damage leads to widespread scarring (fibrosis stage F4). Common causes include chronic hepatitis B or C, long-term alcohol use, and NAFLD/NASH. Many people live with compensated cirrhosis for years without symptoms, but decompensation — when the liver can no longer function adequately — requires urgent medical management.
Compensated vs. Decompensated Cirrhosis
The distinction between these two stages is critical for prognosis and treatment planning.
- •Compensated: The liver is scarred but still functioning. Patients may have no symptoms. Focus is on preventing progression.
- •Decompensated: The liver can no longer perform essential functions. Signs include ascites (fluid buildup), variceal bleeding, hepatic encephalopathy, and jaundice.
- •Once decompensation occurs, transplant evaluation becomes a priority.
Common Causes
Cirrhosis can result from many types of chronic liver injury:
- •Chronic Hepatitis C (most common cause historically)
- •Chronic Hepatitis B
- •Alcohol-related liver disease
- •NAFLD/NASH (fastest growing cause)
- •Autoimmune hepatitis
- •Primary biliary cholangitis (PBC)
- •Primary sclerosing cholangitis (PSC)
- •Wilson's disease, hemochromatosis, and other genetic conditions
Complications to Watch For
Cirrhosis patients need regular screening for these potentially life-threatening complications:
- •Portal hypertension and esophageal/gastric varices
- •Ascites (abdominal fluid) and spontaneous bacterial peritonitis (SBP)
- •Hepatic encephalopathy (confusion, cognitive changes)
- •Hepatocellular carcinoma (HCC) — liver cancer screening every 6 months
- •Hepatorenal syndrome (kidney failure)
- •Coagulopathy (bleeding disorders due to impaired clotting factor production)
Treatment & Management
While cirrhosis itself cannot be reversed, its progression can be slowed and complications managed:
- •Treat the underlying cause (antiviral therapy for hepatitis, abstinence from alcohol)
- •Regular variceal screening via upper endoscopy
- •HCC surveillance with ultrasound and AFP every 6 months
- •Diuretics for ascites management
- •Lactulose and rifaximin for hepatic encephalopathy
- •Liver transplant evaluation when MELD score indicates
- •Avoid all hepatotoxic substances including NSAIDs and certain supplements
Key Labs to Track
MELD Score (Bilirubin, Creatinine, INR)
The primary score used for transplant prioritization. Tracks disease severity over time.
Albumin
Low albumin indicates impaired liver synthetic function. Key component of Child-Pugh score.
Platelet Count
Low platelets suggest portal hypertension and advanced fibrosis.
INR / PT
Measures clotting ability. Elevated INR indicates impaired liver function.
Bilirubin
Rising bilirubin signals worsening liver function and possible decompensation.
Sodium
Low sodium (hyponatremia) is common in advanced cirrhosis and affects MELD-Na score.
AFP (Alpha-Fetoprotein)
Tumor marker for hepatocellular carcinoma. Checked every 6 months.
Creatinine
Kidney function monitoring — hepatorenal syndrome is a serious complication.
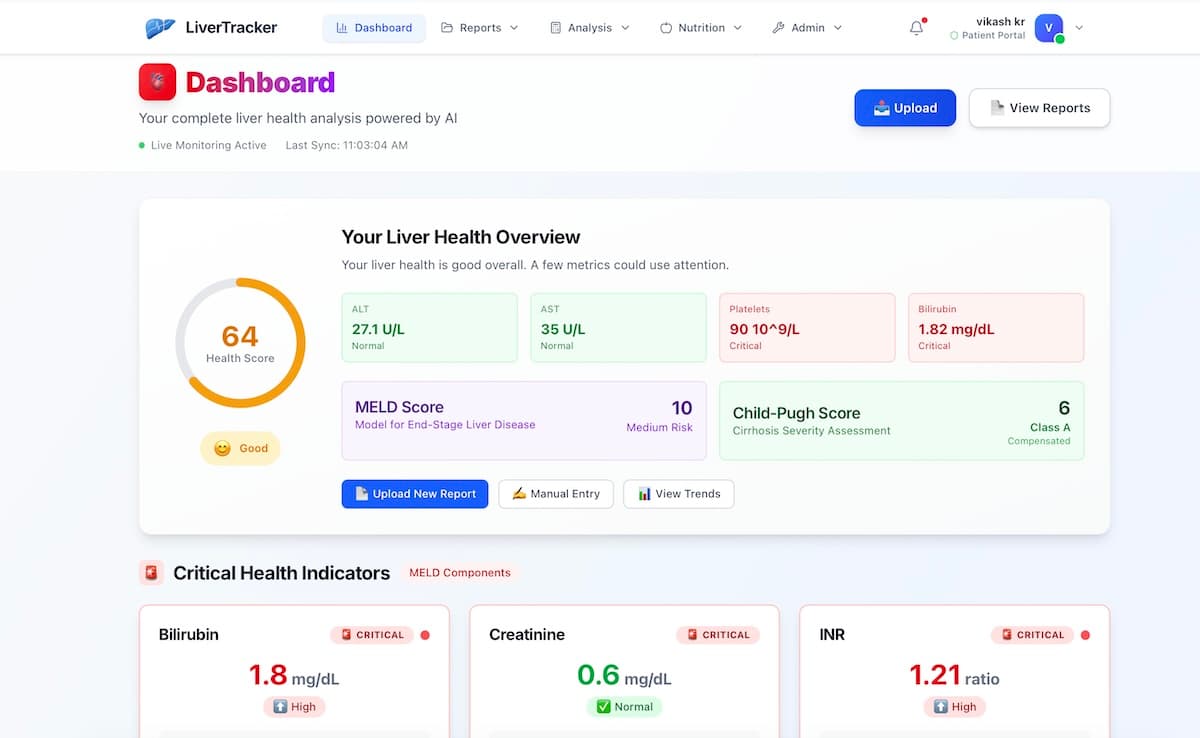
How LiverTracker Helps
Automatic MELD, MELD-Na, and MELD 3.0 score calculation from your labs
Child-Pugh score tracking to monitor compensated vs. decompensated status
Trend charts showing bilirubin, albumin, INR, and platelet changes over time
AI alerts when lab values suggest worsening liver function
FibroScan score tracking and fibrosis stage visualization
One-click report sharing with your transplant team
Imaging findings tracking for varices, ascites, and HCC surveillance
See Your Data Come to Life
Upload your lab reports and get instant AI-powered insights, trend charts, and health scores.
Frequently Asked Questions
Can cirrhosis be reversed?
In most cases, established cirrhosis (F4 fibrosis) cannot be fully reversed. However, treating the underlying cause can halt progression and even allow some regression of fibrosis. Early-stage cirrhosis has better outcomes than decompensated disease.
What MELD score means I need a transplant?
Generally, a MELD score of 15 or higher qualifies for transplant listing. Scores above 25 indicate high urgency. LiverTracker calculates your MELD automatically so you can track changes between appointments.
How often should I get labs done with cirrhosis?
Most hepatologists recommend comprehensive labs every 3 months for compensated cirrhosis, and monthly for decompensated. HCC screening (ultrasound + AFP) should be done every 6 months.
What is the difference between MELD and Child-Pugh?
MELD uses bilirubin, creatinine, and INR to predict 3-month mortality and is used for transplant prioritization. Child-Pugh uses bilirubin, albumin, INR, plus clinical factors (ascites, encephalopathy) to classify severity as Class A, B, or C. LiverTracker calculates both.
Related Conditions
Take Control of Your Liver Health
Upload your lab reports, track your progress, and get AI-powered insights — all for free.
Get Started FreeMedical Disclaimer: This page is for educational purposes only and does not constitute medical advice. Always consult your hepatologist or primary care physician for diagnosis and treatment decisions.